Arterial stiffness may be a novel risk factor for metabolic syndrome in teens, a paper published in the American Journal of Physiology-Heart and Circulatory Physiology concludes. The study was conducted in collaboration between the University of Bristol in the UK, the University of Exeter in the UK, and the University of Eastern Finland.
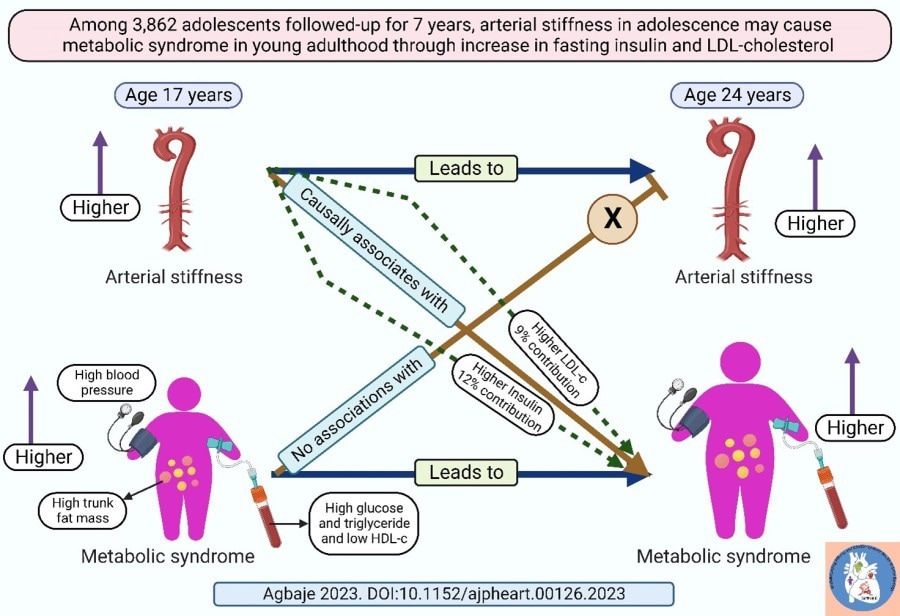
The presence of any three of high blood pressure, high trunk fat mass, high fasting glucose, high fasting triglyceride and low fasting high-density lipoprotein cholesterol describes metabolic syndrome. Arterial stiffness in adolescents measured with carotid-femoral pulse wave velocity may potentially cause metabolic syndrome in young adulthood via an increase in fasting insulin resistance and low-density lipoprotein cholesterol. Image Credit: Andrew Agbaje.
The World Health Organization describes metabolic syndrome as the constellation of three or more of the following: abdominal obesity, insulin resistance, hypertension, and hyperlipidemia. The prevalence of metabolic syndrome in US middle-aged adults is 30%, increasing to 50% in adults older than 60 years. In Finland, the prevalence of metabolic syndrome is 30% in men and 25% in women. Metabolic syndrome increases the risk of worsening obesity, type 2 diabetes, cardiovascular disease, and premature death.
Already among children aged 6 – 12 years, the prevalence of metabolic syndrome is approximately 3% while among adolescents aged 13 – 18 years, the prevalence is approximately 5% globally. Among children who are overweight, the prevalence of metabolic syndrome is 12% but 29% among children who are obese. This trend in the prevalence of metabolic syndrome is consistent across the globe; hence the need to identify novel causes and prevent or reverse the disease.
A new risk factor for childhood and adolescent metabolic disease such as obesity and insulin resistance is arterial stiffness. This risk factor is being established as a potential cause of type 2 diabetes among adults globally. However, it is not clear whether arterial stiffness causes metabolic syndrome.
The current study included 3,862 adolescents (1,719 males and 2,413 females) aged 17 years who were followed up until age 24 years. These adolescents had dual-energy Xray absorptiometry measurement for trunk fat mass and skeletal muscle mass, as well as fasting blood samples such as glucose, insulin, high-density lipoprotein cholesterol, low-density lipoprotein cholesterol, triglyceride, and high sensitivity C-reactive protein, in addition to smoking status, socio-economic status, family history of cardiovascular disease, and moderate-to-vigorous physical activity. Arterial stiffness was measured with carotid-femoral pulse wave velocity and the presence of any three of high blood pressure, high trunk fat mass, high fasting glucose, high fasting triglyceride, or low fasting high-density lipoprotein cholesterol was considered to describe metabolic syndrome.
The prevalence of metabolic syndrome in the study was 5% in males and 1.1% in females at age 17 years but 8.8% in males and 2.4% in females at age 24 years. This significant sex-difference in the prevalence of metabolic syndrome is due to a higher proportion of males having elevated systolic blood pressure, hyperglycemia, elevated triglyceride, and reduced high-density lipoprotein cholesterol compared to females. However, females had significantly higher trunk fat mass than males.
During the 7-year follow-up, worsening arterial stiffness was associated with a 9% risk of metabolic syndrome in males but there was no statistically significant risk among females. It was also observed that arterial stiffness potentially caused metabolic syndrome; however, metabolic syndrome did not cause arterial stiffness. The pathway through which arterial stiffness caused metabolism syndrome could be partly explained by an increase in fasting insulin (12% contribution) and low-density lipoprotein cholesterol (9% contribution).
We are seeing for the first time that arterial stiffness in adolescents is an unknown risk factor for metabolic syndrome which may initiate a cascade of disease processes that might lead to type 2 diabetes, cardiovascular disease, and premature death. Early intervention might likely reduce high fasting insulin and low-density lipoprotein cholesterol thereby cutting off 20% of the potential causal effect of arterial stiffness on metabolic syndrome.”
Andrew Agbaje, Physician and Clinical Epidemiologist, University of Eastern Finland
“Pending when randomized clinical trials will be successful in reversing and treating arterial stiffness, it is expedient for caregivers, pediatricians, public health experts, and policymakers to focus on ways to reduce high fasting insulin or insulin resistance and low-density lipoprotein cholesterol, particularly from adolescence through improvement in diet and physical activity,” Agbaje continues.
Dr Agbaje’s research group (urFIT-child) is supported by research grants from Jenny and Antti Wihuri Foundation, the Finnish Cultural Foundation Central Fund, the Finnish Cultural Foundation North Savo Regional Fund, the Orion Research Foundation sr, the Aarne Koskelo Foundation, the Antti and Tyyne Soininen Foundation, the Paulo Foundation, the Yrjö Jahnsson Foundation, the Paavo Nurmi Foundation, the Finnish Foundation for Cardiovascular Research and the Foundation for Pediatric Research.
Source: